PROCEDURES
DISCOVER YOUR IDEAL FACELIFT®
COSMETIC SURGERY HAS NEVER BEFORE ENJOYED SO MUCH POPULARITY, OR OFFERED SO MANY OPTIONS TO HELP WOMEN AND MEN ACHIEVE YOUTHFUL LOOKS, FEATURES AND FIGURES THEY DESIRE.
PHOTOS OF PATIENTS WITH A BREAST AUGMENTATION
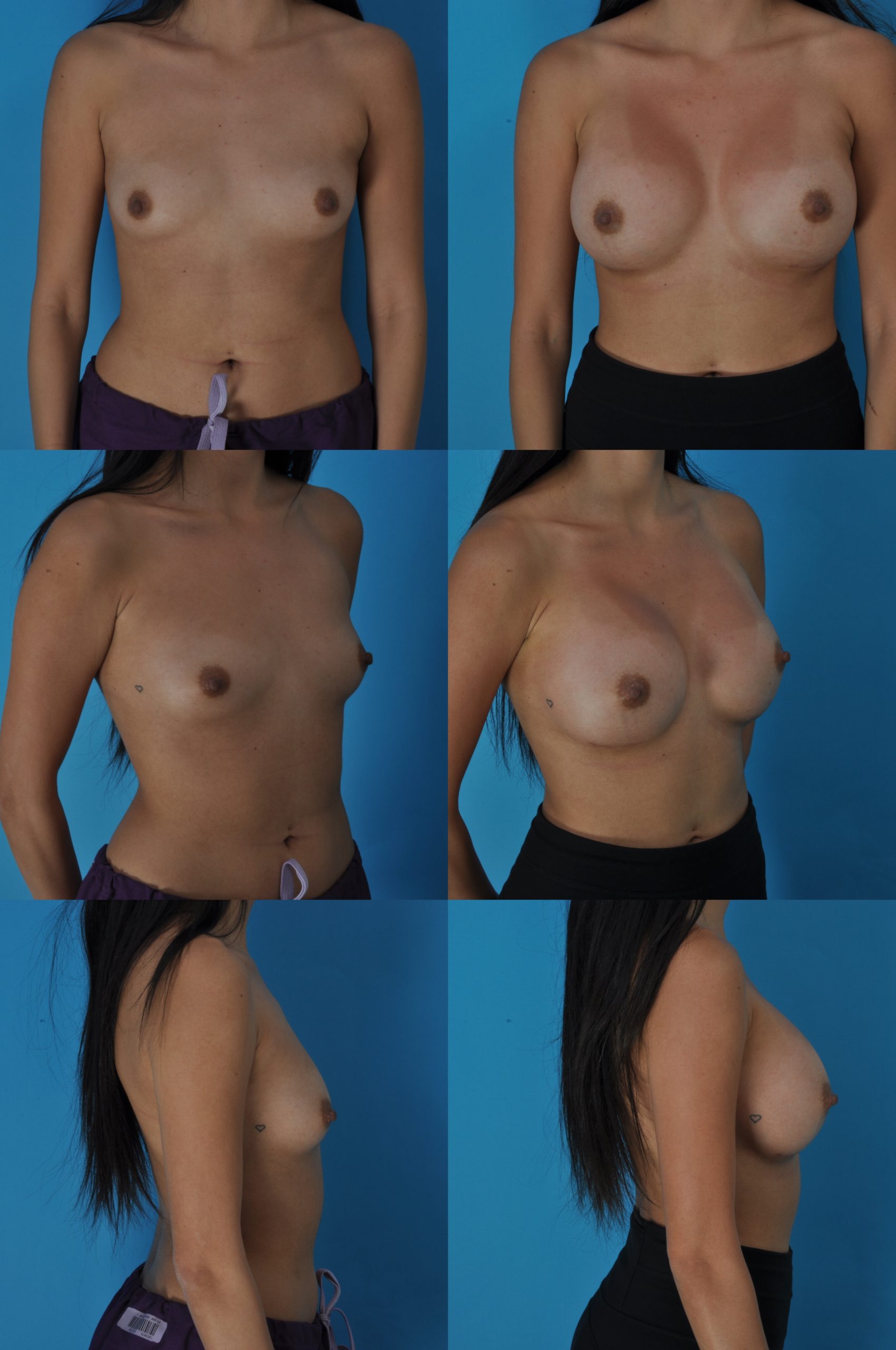
Implant Size: Right Breast: 450 cc/Left Breast: 450cc
A.E.
Age: 25
Height: 5’2 ”
Weight: 110 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Type: Silicone Implants
Before, 2 months after

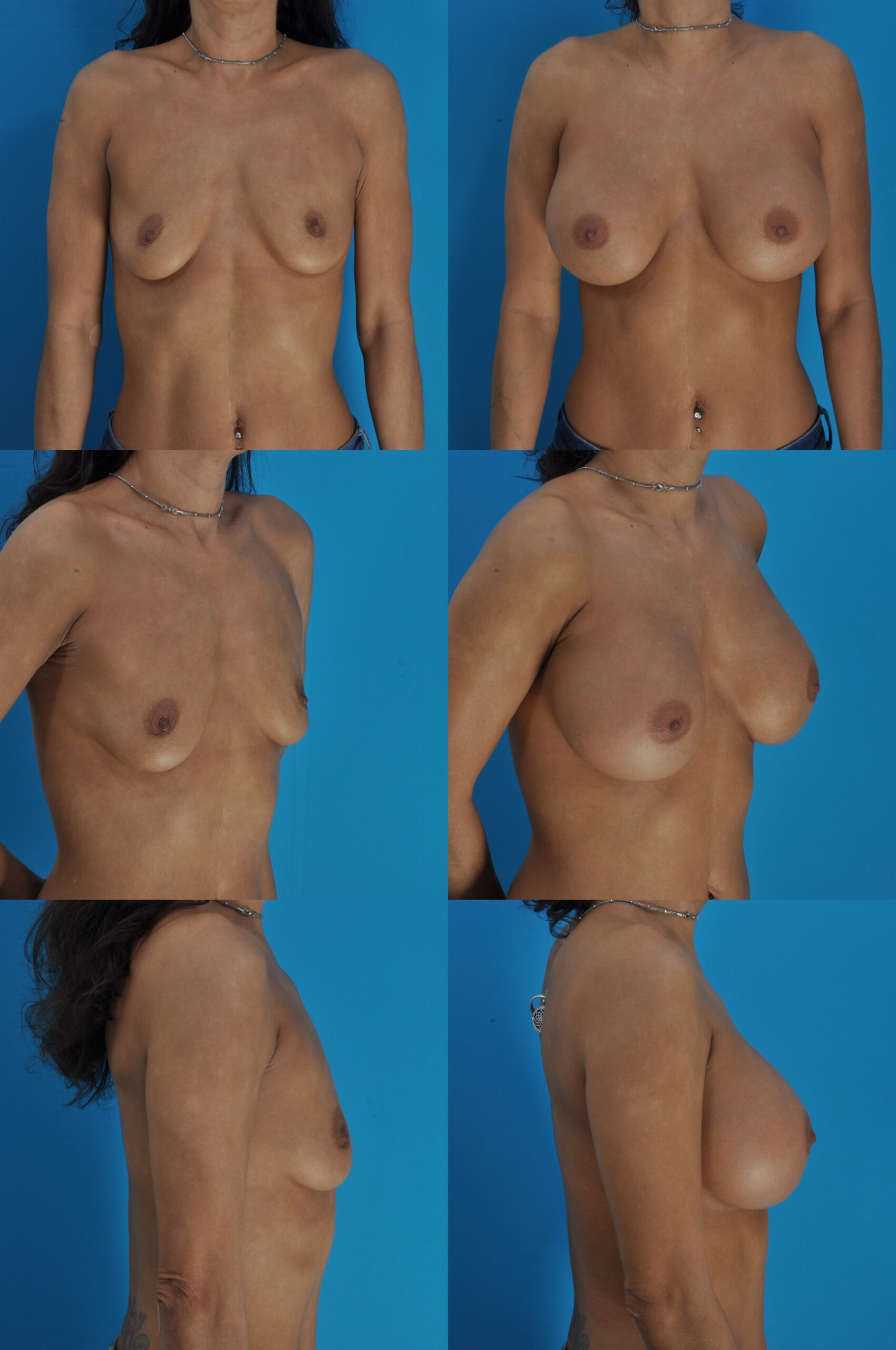
Implant Size: 450 cc
T.H.
Age: 23
Implant Type: Silicone Gel
Before, 3 months after

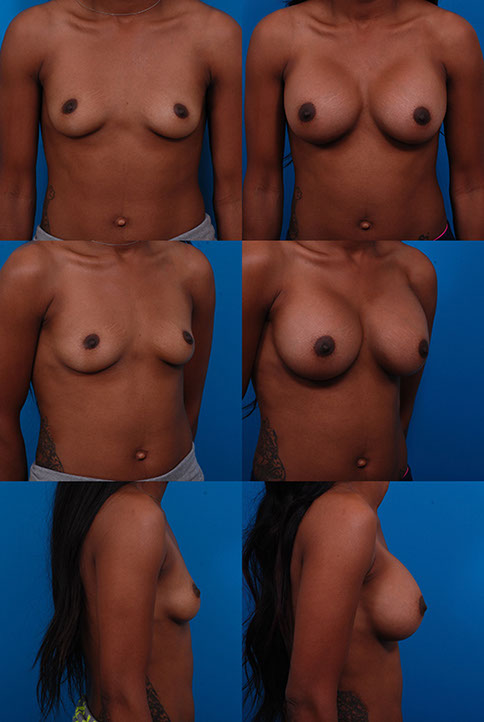
Implant Size: Right Breast: 420 cc/Left Breast: 420 cc
K.H.
Age: 27
Height: 5’3″
Weight: 121 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Type: Saline
Before, 3 weeks after

Implant: 375 cc
C.S.
Age 34
Implant type: Mentor high-profile silicone gel
Placement: Subpectoral
1 month

Implants: Right 400 cc, Left 425 cc
S.B.
Age 36
Implant Type: Silicone Gel
1 month
Implants: 450 cc
K.R.
Age: 41
Implant Type: Silicone Gel
3 months
Prepectoral (above the muscle)
Z.B., Age 24
Implant: 415 cc silicone gel
Note: This bodybuilder requested implant placement above the muscle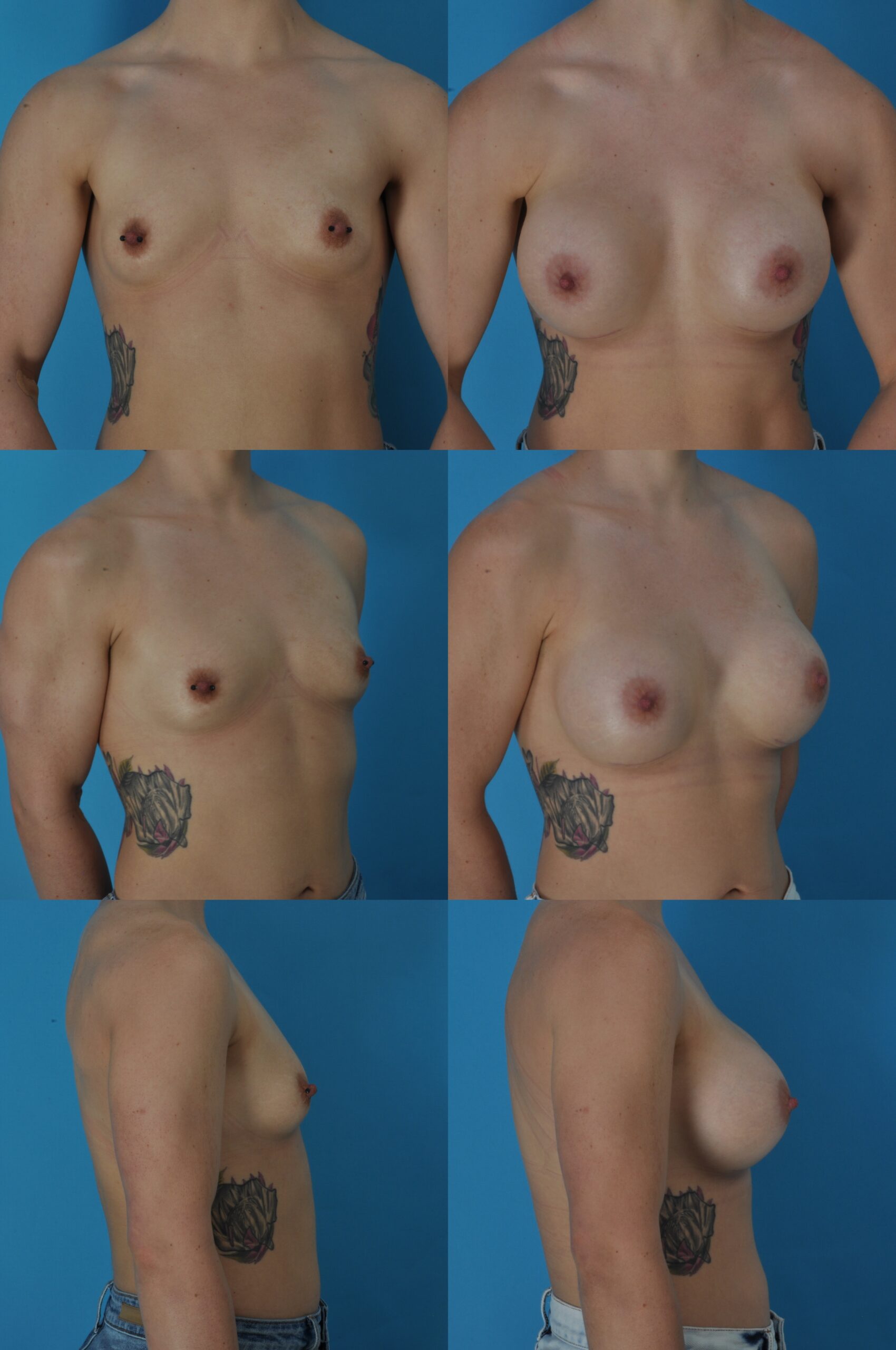
Prepectoral
Large Chest Size
B.K., Age 28
Implant: 600 cc silicone gel
3 months
Replacement with a Larger Size Implant
K.L., Age 29/41
450 cc saline, then 800 cc silicone gel
12 years after first procedure, 3 months after second procedure
M.H., Age 19/28
420 cc saline, then 800 cc saline
8 years after first procedure, 5 weeks after second procedure
Average Chest Size
L.B., Age 26
Height: 5’4″
Weight: 114 lbs.
Implant Type: Mentor smooth, round, moderate-plus profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 350 cc/Left Breast: 360 cc
Before, 6 months after
Q.J., Age 36
Implant Size: 425 cc silicone gel
3 months
J. M., Age 38
Implants: 375 cc silicone gel
1 month
A.B., Age 47
500 cc silicone gel
3 months
Nipple Reduction
V.A., Age 43
Height: 5’3″
Weight: 136 lbs.
Implant Type: Allergan Natrelle smooth, round, moderate profile, saline-filled
Placement: Submuscular
Incision: Trans-Nipple
Implant Size: 360 cc
Before, 3 months after
M.V., Age 45
Height: 5’3″
Weight: 125 lbs.
Implant Type: Allergan Natrelle smooth, round, silicone gel
Placement: Submuscular
Incision: Inframammary
Implant Size: 397 cc

M.V. Age 45 Height: 5’3″ Weight: 125 lbs. Implant Size: 397 cc
Before, 5 years after
A.C., Age 24
Height: 5’6″
Weight: 123 lbs.
Implant Type: Mentor smooth, round, moderate-plus profile, silicone gel
Placement: Submuscular
Incision: Inframammary
Implant Size: 400 cc

A.C. Age 24 Height: 5’6″ Weight: 123 lbs. Implant Size: 400 cc
Before, 2 months after
Large Implant Size, With Nipple Elevation On One Side
Y.C., Age 27
To improve symmetry, a right nipple elevation was done, using a “crescent” mastopexy to adjust the position of the right nipple and areola. The scar is still red and noticeable, but will fade over time.
Height: 5’1″
Weight: 105 lbs.
Implant Type: Allergan Natrelle smooth, round, moderate profile, saline-filled
Placement: Submuscular
Incision: Inframammary
Implant Size: Right Breast: 500 cc/Left Breast: 510 cc

Y.C. Age 27 Height: 5’1″ Weight: 105 lbs. Size: Right Breast: 500 cc/Left Breast: 510 cc Note: To improve symmetry, a right nipple elevation was done, using a “crescent” mastopexy to adjust the position of the right nipple and areola. The scar is still red and noticeable, but will fade over time.
Before, 2 months after
A.G., Age 40
Height: 5’2″
Weight: 150 lbs.
Implant Type: Mentor MemoryGel smooth, round, moderate-plus profile, silicone gel
Placement: Submuscular
Incision: Inframammary
Implant Size: 600cc
Before, 3 months after
T.A. Age 27
Height: 5’1″
Weight: 110 lbs.
Implant Type: Sientra smooth, round, moderate profile, silicone gel
Placement: Submuscular
Incision: Inframammary
Implant Size: 385 cc
T.A. Age 27 Height: 5’1″ Weight: 110 lbs. Implant Size: 385cc
Before, 3 months after
J.M., Age 25
Breast Augmentation.
Height: 5’3″
Weight: 136 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 500 cc/Left Breast: 500 cc
Silicone Implants

J.M., Age 25 Breast Augmentation. Height: 5’3″ Weight: 136 lbs. Implant Size: 500cc
Before, 2 years after
Mommy Makeover
S.M., Age 28,
Height: 5’2″
Weight: 128 lbs.
Implant Type: Mentor smooth, round, moderate-plus profile, silicone gel
Placement: Submuscular
Incision: Periareolar
Implant Size: Right Breast: 425 cc/Left Breast: 400 cc

S.M. Age 28 Height: 5’2″ Weight: 128 lbs. Incision: Periareolar Implant Size: Right Breast 425 cc/Left Breast 400 cc
Before, 3 years after
L.C., Age 28
Height: 5’4″
Weight: 129 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 300 cc/Left Breast: 300 cc
Silicone Implants

L.C. Age 28 Height: 5’4″ Weight: 129 lbs. Implant Size: 300cc
J.R., Age 36
This patient developed a left breast capsular contracture that was released 3 years after surgery.
Height: 5’6″
Weight: 133 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 360 cc/Left Breast: 360 cc
Saline Implants
Before, 2 months after 2nd procedure
J.L., Age 39
Height: 5’4″
Weight: 129 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 425 cc/Left Breast: 425 cc
Silicone Implants
Before, 3 months after
PHOTOS OF PATIENTS WITH A PERIAREOLAR INCISION
P.B., Age 23
Height: 5’3″
Weight: 105.5 lbs.
Implant Type: Mentor smooth, round, moderate profile, saline-filled
Placement: Submuscular
Approach: Periareolar
Implant Size: Right Breast: 330 cc/Left Breast: 325 cc



Close-up of periareolar scar
L.B., Age 28
Height: 5’4″
Weight: 123 lbs.
Placement: Submuscular
Approach: Periareolar
Implant Size: Right Breast: 350 cc/Left Breast: 350 cc
Silicone Implants

Before, 3 months after
P.S., Age 30
Height: 5’4″
Weight: 115 lbs.
Placement: submuscular
Approach: Periareolar
Implant Size: 390cc
Saline Implants

Before, 3 months
D.A. Age 33,
Height: 5’5″
Weight: 150.5 lbs.
Implant Type: Mentor smooth, round, moderate-plus profile, saline-filled
Placement: Submuscular
Approach: Periareolar
Implant Size: Right Breast: 400 cc/Left Breast: 420 cc

Before, 6 weeks after
PHOTOS OF PATIENTS WITH COLLAPSED NIPPLE/AREOLAS
K.S., Age 41
Height: 5’9″
Weight: 158 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 440 cc/Left Breast: 450 cc
Saline Implants

Before, 21 months after
PHOTOS OF PATIENTS WITH TREATABLE ASYMMETRY
B.S., Age 20
Height: 5’8″
Weight: 126 lbs.
Implant Type: Mentor smooth, round, moderate profile, saline-filled
Placement: Submuscular
Incision: Inframammary
Implant Size: Right: 370 cc/Left: 425 cc

Before, 1 month after
Mild Asymmetry
K.E., Age 19
Height: 5’8″
Weight: 124 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 450 cc/Left Breast: 450 cc
Saline Implants

Before, 1 year after
V.G., Age 19
Height: 5’7″
Weight: 156 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 450 cc/Left Breast: 450 cc
Saline Implants

Before, 5 months after
A.D., Age 22
Height: 5’7″
Weight: 124 lbs
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 480 cc/Left Breast: 450 cc
Saline Implants

Before, 21 months after
J.D., Age 28
Height: 4’9″
Weight: 162 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 480 cc/Left Breast: 360 cc
Saline Implants

Before, 3 years after
T.B., Age 29.
Breast augmentation with right periareolar mastopexy and left vertical mastopexy. 3 months
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 520 cc/Left Breast: 550 cc
Saline Implants

Before, 3 months after
K.M., Age 32
Height: 5’6″
Weight: 125 lbs.
Implant Type: Allergan Natrelle smooth, round, moderate profile, saline-filled
Placement: Submuscular
Incision: Inframammary
Implant Size: Right Breast: 420 cc/Left Breast: 400 cc

Before, 1 month after
L.G., Age 32
Height: 5’1 “
Weight: 115 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 375 cc/Left Breast: 275 cc
Silicone Implants

Before, 3 months after
PHOTOS OF PATIENTS OVER 50
M.C.
Age 52
Height:5 ‘2 “
Weight: 115 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast:300 cc/Left Breast:300 cc
Saline Implants

Before, 3 months after
C.M., Age 57
Height: 5’5 “
Weight: 140
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 550cc/Left Breast: 550cc Silicone

Before, 3 months after
PHOTOS OF PATIENTS WITH TUBEROUS AND NARROWLY BASED BREASTS
J.A., Age 27
Height: 5’7″
Weight: 143 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 420 cc/Left Breast: 420 cc
Silicone Implants

Before, 1 month after
S.G., Age 32
Height: 5’4″
Weight: 130 lbs.
Placement: Submuscular
Approach: Periareolar incision
Implant Size: Right Breast: 420 cc/Left Breast: 420 cc
Saline Implants

Before, 3 months, 7 years after
PHOTOS OF PATIENTS WITH SAGGING BREASTS TREATED WITH IMPLANTS ALONE
R.G. Age 30
Height: 5’7 “
Weight: 142 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 420 cc/Left Breast: 420cc
Saline Implants

Before, 3 months after
W.B. Age 30
Height: 5’4″
Weight: 114.5 lbs.
Implant Type: Mentor smooth, round, moderate profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 475 cc/Left Breast: 480 cc

Before, 10 months after
B.N. Age 32
Implant Type: Moderate-plus profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 470 cc / Left Breast: 480 cc

Before, 3 months after
PHOTOS OF PATIENTS WITH IMPLANTS SETTLING OVER TIME
C.C., Age 30
Height: 5’5″
Weight: 116
Placement: Submuscular
Approach: Inframammary
Implant size: 450 cc
Implant type: Mentor smooth, round, moderate plus profile, saline-filled
Before, 1 month, 3 months, 7½ years after

3 months after
D.U., Age 33
Height: 5’6″
Weight: 131.5
Implant type: McGhan smooth, round, moderate-profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant size: 330 cc

Before, 1 month after, 3 months after
B.M., Age 33
Height: 5‘10½”
Weight: 141
Implant Type: Mentor smooth, round, moderate profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 400 cc

Before, 1 month after, 1 year after
T.C., Age 34
Height: 5’3″
Weight: 124
Implant Type: Mentor smooth, round, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 400 cc

Before, 6 weeks after, 15 years after
R.H., Age 43
Height: 5’4″
Weight: 130
Implant type: Mentor smooth, round, moderate-plus profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant size: 400 cc

Before, 1 month after, 3 months after
J.K., Age 26 and 36
Height: 5’5″
Implant Type: McGhan round, moderate profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 400 cc

Before, 6 weeks after, 10 years after
PHOTOS OF PATIENTS WITH IMPLANTS—SMALLER TO LARGER

Before, 9 months after
J.H., Age 31
Height: 5’6″
Weight: 148 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 310 cc/Left Breast: 290 cc Saline

Before, 1 month after

Before, 5 weeks after

Before, 6 weeks after
Implants After Multiple Pregnancies

Before, 1 month after

Before, 6 weeks after

Before, 3 months after

Before, 3 months after

Before, 3 months after
L.B., Age 32
Height: 5’4″
Weight: 110 lbs.
Implant Type: Mentor smooth, round, moderate profile, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 425 cc/Left Breast: 435 cc

Before, 3 months after

Before, 3 months after
PHOTOS OF PATIENTS WITH LARGE IMPLANT SIZES
D.W-R., Age 23
Height: 5’4″
Weight: 168 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 550 cc/Left Breast: 550 cc
Saline Implants

Before, 3 months after
J.B., Age 22 and 29
Height: 5’3″
Weight: 120 lbs.
Implant Type: (1) Mentor smooth, round, moderate-plus profile, saline-filled (2) Allergan smooth, round, moderate profile, Inspira silicone gel
Placement: Submuscular
Incision: Inframammary
Implant Size: (1) 360 cc, (2) 640 cc

Before, 5 months after first augmentation (360 cc) and then 2½ months after replacement with larger implants (640 cc) 7 years later.
E.H. Age 27
Height: 5’5 “
Weight: 143 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 500cc/Left Breast: 500cc
Silicone Implants

Before, 3 months after
A.L., Age 35
Height: 5’3″
Weight: 114 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 500 cc/Left Breast: 500 cc
Silicone High Profile Implants

Before, 3 months
PHOTOS OF PATIENTS WITH INDIVIDUALIZED BREAST CONDITIONS
Pigeon Chest (“Pectus Carnae”)
C.B., Age 27
Procedure: Breast Augmentation
Height: 5’4″
Weight: 108 lbs.
Implant Type: McGhan round, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 375 cc

Before, 7 weeks after
Tuberous Breasts
G.M., Age 29
Height: 5’7″
Weight: 142 lbs.
Implant Type: Mentor smooth, round, saline-filled.
Placement: Submuscular
Approach: Trans-Nipple
Implant Size: 400 cc

Before, 14 months after
Sunken Chest (“Pectus Excavatum”)

Before, 6 weeks after
Stretch Marks
Women often ask if breast implants cause stretch marks. One would think that the tension created by inserting breast implants might cause stretch marks. Fortunately, implants themselves do not usually cause stretch marks.
In fact, we do not know why some women are prone to developing stretch marks after pregnancy or weight loss, or just by virtue of having larger breasts. Certainly there is a genetic predisposition. Whatever skin changes have occurred to cause the development of stretch marks in the past, or possibly will occur in the future, these changes seem to go on regardless of the presence of implants. Existing stretch marks are not improved by the augmentation, but they are not made worse either. The breasts look better anyway, and the stretch marks can be less obvious because the tone of the skin is improved by taking up the slack, making any contour depressions caused by stretch marks less visible.
J.V., Age 33
Height: 5’7″
Weight: 130 lbs.
Implant Type: McGhan, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 380 cc

Before, 1 year after
Collapsed Nipples
K.A., Age 35
Height: 5’0″
Weight: 103 lbs.
Implant Type: Mentor round, saline-filled
Placement: Submuscular
Approach: Inframammary
Implant Size: 300 cc

Before, 3 months after
Over projecting Nipples
J.V., Age 40
Height: 5’2″
Weight: 84 lbs.
Implant Type: Mentor smooth, round, moderate-plus profile, saline-filled
Placement: Submuscular
Approach: Trans-Nipple
Implant Size: 270 cc

Before, 3 months after

Close-up of incision
Inverted Nipples
H.C., Age 24
Height: 5’7″
Weight: 117 lbs.
Placement: Submuscular
Approach: Trans-Nipple
Implant Size: 380 cc
Implant Type: Mentor smooth, round, moderate profile, saline-filled

Before, 4 weeks after
PHOTOS OF PATIENTS THAT TRANSITION FROM MALE TO FEMALE
C.M., Age 23
Implant Type: (1) Saline-filled (2) Natrelle smooth, round high profile saline-filled
Placement: Submuscular
Incision: Inframammary
Implant Size: (1st procedure) 400 cc, (2nd procedure) 900 cc
![]()
Before, 1 month after the second operation
PHOTOS OF PATIENTS WITH REPAIR OF EXISTING DEFORMITIES AFTER PREVIOUS BREAST AUGMENTATION
A.G., Age 21
Procedure: Replacement of breast implants and capsular repairs. This patient had 2 previous breast augmentations previously, performed elsewhere. Her existing implants were replaced with a larger size and both capsules were released medially and superiorly and reinforced laterally and inferiorly.
Height: 5’7″
Weight: 135 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 457 cc/Left Breast: 457 cc
Silicone Implants

Before, 1 year after
A.W., Age 36
Procedure: Replacement of breast implants and capsular repairs. This patient had a previous breast augmentation performed elsewhere and a previous attempted correction of symmastia and bottoming out.
Height:5’6″
Weight: 148 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast:450 cc/Left Breast:450 cc
silicone Implants

Before, 3 months after
S.U., Age 37
Breast augmentation with lateral capsular repairs and removal of accessory nipple from left breast. This patient had a breast augmentation elsewhere 7 years previously.
Height:5’4″
Weight: 141 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast:600 cc/Left Breast:600 cc
Silicone High profile Implants

Before, 3 months after
L.D., Age 42
Revision of breast augmentation. This patient had a breast augmentation 7 months previously. Her left side showed bottoming out. The capsules on both sides were adjusted.
Height:5’7″
Weight: 144 lbs.
Placement: Submuscular
Approach: Inframammary
Implant Size: Right Breast: 475cc/Left Breast: 475cc
Silicone Implants

Before, 7 months, 3 months after 2nd procedure
PHOTOS OF PATIENTS WITH REMOVAL OF BREAST IMPLANTS
J.W., Age 29
Procedure: Removal of breast implants. This patient wanted to have her implants removed because of personal preference. She ran a half marathon 3 weeks later.

Before, 1 month after
SELECT YOUR AREA OF INTEREST:
YOUR IDEAL FACELIFT®
The Evolution of Facelifts
Unfortunately, the word “facelift” may conjure unflattering images of aging actresses with unnatural expressions—the skin pulled tight and the corners of the mouth pulled toward the ears. This is not a desirable appearance. No one wants to look artificial or freakish. In fact, most people prefer to look like themselves, just without the superimposed effects of aging, which make them look less like themselves. Family members may respond negatively to “Mom” wanting a facelift. Spouses, nervous about the idea, tell their partners they love them the way they are. Patients deal with guilt feelings, as if their desire for a more youthful appearance were a frivolous self-indulgence.
This unfortunate reputation is not undeserved. Those who have had facelifts in the past, or second and third facelifts, with excessive skin tightening, often do have an unnatural look. Not a younger look, just a “lifted” look. Sometimes this appearance can be seen across the room. Importantly, this outcome is not a necessary consequence of a facelift itself, but a consequence of facelifts that stretch the skin tight, instead of repositioning the foundation layer (SMAS) below it. Contrary to conventional wisdom, an unnatural-looking outcome is not a consequence of patient vanity or having “too much done.” Rather, it is a failure of technique.
The pioneers in plastic surgery were well-aware that skin lost elasticity with age and tended to sag with gravity. It was understandable that they would seek to restore a youthful appearance by tightening the facial skin. The first facelift was performed in 1901. The original, antiquated term was “rhytidectomy,” which means to literally cut out the wrinkles. The appearance of the jawline and neck was improved, but patients still looked older in the midface (cheek areas). The procedure improved the neckline, but did little to correct the nasolabial creases—the parentheses, ( ), caused by sagging cheek tissue. After surgery, these patients often looked like a fifty-something who had a facelift, rather than the desired forty-something. Treatment of the midface became the challenge for plastic surgeons.
Facelifts in the 1980s and 1990s
Inspired by the work of Dr. Tord Skoog, who first incorporated a deeper tissue level in his facelifts, plastic surgeons In the 1980s and 1990s started performing deep plane (sub-SMAS) facelifts that elevated the connective tissue plane under the skin. “SMAS” is an acronym for “superficial musculoanoneurotic system.” It is a wordy term that describes the connective tissue layer under the skin that is continuous with the frontalis muscle in the forehead and the platysma muscle in the neck. Sometimes the SMAS is called the “muscle layer,” although it is made up of inelastic connective tissue in the face. In deep plane facelifts, the tension is applied to this deeper tissue layer, which is relatively strong and unlikely to stretch, avoiding tension on the skin. The skin comes up with this deeper layer. The fat, sandwiched between the SMAS and the skin, comes up too (See Illustration). By releasing and repositioning the SMAS, all three tissue layers of the midface—connective tissue, fat, and skin—are elevated.
Fat is injected into the plane between the skin and the SMAS, restoring cheek fullness. By releasing the SMAS and using it as a handle, the skin and the fat layer between the skin and the SMAS are elevated with it, avoiding skin tension that might otherwise create an operated look. This tissue elevation produces a temporary bump in the temple that flattens on its own. An additional incision is avoided.
How Do You Know If You Are Ready for a Facelift?
It takes courage to see a plastic surgeon. It is impossible to miss media coverage of plastic surgery and facelifts graphically presented on prime time TV and the internet. Many of my patients ask about celebrities who had plastic surgery. They don’t want to end up looking weird. They are worried about the reactions of friends and family. They feel guilty about spending money on themselves. Yet, they still work up the nerve. That patients arrive at my office despite all of these influences speaks to the profound unhappiness that faces them (literally) every time they look in the mirror. One older patient of mine who lived alone confided that she had all the mirrors in her house taken down. I thought she was kidding at first, but she was serious.
The facelift improves the tone of the face. Hereditary factors and aging cause gradual relaxation of the facial tissues. The skin loses elasticity and gravity accentuates the sagging. Most of my patients observe this process over a period of several years. Others say it seemed to happen almost overnight. They may pull their skin back when looking in the mirror to demonstrate how much the skin has loosened.
There is no specific age for having a facelift. My youngest facelift patient was 33 and the oldest 85. A common age is around 50. Most women are noticing jowls at this age. Also, this may be a watershed time in their lives—the onset of middle age with grown-up children and perhaps finally the opportunity to do something for oneself rather than others. Sometimes patients are motivated by a marital breakup, substantial weight loss, change in job, retirement, or moving to a new city. But there is no ideal age for a facelift and likewise no reason to delay the surgery until a certain numerical age.
The decision to take action is not a hurried one. On the contrary, patients think about it for a long time. Our experience is that facelift patients consider the surgery for an average of 3 or 4 years before having it (Swanson E. Outcome analysis in 93 facial rejuvenation patients treated with a deep-plane face lift. Plast Reconstr Surg. 2011;127:823–834).
In considering timing for surgery, physical findings—loose skin, sagging cheeks, and jowls—are more important than chronological age itself. When these signs of aging start causing concern, a facelift may be recommended, whether the patient is 45 or 55. I have patients in my practice who were ready for a facelift at age 42 (See C.C. in Patient Photographs). Others may make it into their 50s before their skin tone has loosened enough to need a facelift. There are very few genetically-advantaged women who would not benefit from a facelift by their mid-50s. It amuses plastic surgeons to hear celebrities claim they have no interest in cosmetic surgery in their 40s; invariably, they come to another conclusion one morning while looking in the mirror in their 50s. Mothers say to their disapproving daughters, “Just you wait.”
There are advantages in not waiting once the signs of aging are apparent. Having a facelift earlier rather than later, while the skin still has greater elasticity, avoids deeper creases that can be more difficult to treat later on. With proper skin care (i.e., sun protection) and future touch-up procedures as needed, many patients can maintain an appearance much younger than their chronological age well into their later years—a “50,000 mile overhaul” followed by tune-ups, so to speak.
Patients who decide to have a facelift may say to me, “I love my mother, but I don’t like seeing her when I look in the mirror.” Or, “I’m getting that jowly, double-chinned look that runs in my family and that crease along the side of my nose.”
Often an important family event such as a wedding or a reunion, for example, provides the impetus to make changes. Patients may see their facial profile in photographs and are surprised at how they look, not knowing that “it had gotten that bad.”
Many patients tell me that their spouses are supportive, but hesitant. “He tells me he loves me just the way I am. But I’m doing this for me.” These words tell me the patient is ready and has the right motivation. She is doing it to feel better about herself, not to please others.
You might be a candidate if:
- You don’t like looking down because your jowls sag more.
- When looking in the mirror, you pull up on your face with a finger on each temple to take up the slack in the skin.
- You don’t like the appearance of loose skin or vertical bands of the neck.
- You don’t like how you’re starting to look in pictures, particularly profile views.
- You feel like you’re finally looking like your parents.
- Your aging appearance is starting to affect your mood and self-esteem.
What Causes Facial Aging?
Typically, skin laxity starts to become noticeable in one’s early 40s. Many women today have a facelift in their mid-40s. Patients in their early 50s often tell me, “You know, I was doing alright up until just last year. Then my face just seemed to fall apart.” They may make a correlation with menopause or a stressful life event such as a divorce or loss of a parent.
Genetics are most relevant. For a glimpse of what the future holds, just take a look at your parents or other close relatives. It’s usually not very reassuring.
Sun exposure matters, particularly in light-complected individuals with less ultraviolet protection from melanin, who are therefore more susceptible to “photo-aging.” Fortunately this effect is avoidable with diligent use of sunscreen and hats. Patients should not feel that the damage has already been done and there is little point in changing their habits. In fact, skin quality improves with sun protection, even in middle age. It’s time for hats to make a comeback as a fashion accessory!
Ethnicity and gender make a difference. Thin skin ages faster than thicker skin, which is why women, who have thinner skin, tend to seek treatment at an earlier age than men. People with fair skin types tend to wrinkle more and sag more than darker skin types. In my practice, Caucasians typically have facelifts earlier and more commonly than patients of color.
Does Smoking Matter?
Conventional wisdom holds that the habit of tightening the lips around a cigarette causes more wrinkles to form around the lips, commonly known as smoker’s lines. But these lines develop in plenty of nonsmokers too. Of course, smoking cannot be good for the skin, but whether it affects skin aging is unknown. One thing is certain—smoking interferes with skin circulation. Smoking is to be avoided around the time of surgery because it increases the risk of healing problems.
Reasons for Having a Facelift
Patients wonder if vanity is an acceptable reason for wanting a facelift. An appropriate response may be: “Is it reasonable to buy new clothes, repaint your house, or repair dents and scratches on your car? Why would it not be OK to spruce up your facial appearance?”
People in many parts of the world, Brazil, for example, do not find it necessary to justify having cosmetic surgery. Perhaps it is the heritage that makes Americans feel guilty about this form of self-indulgence, although you would hardly know it judging by the rest of our culture. The purist would eschew jewelry and makeup and leave her hair looking like Albert Einstein’s. But even in Einstein’s day, if you looked like that, you’d better have some good theories. Even Popes enjoy wearing Prada shoes and Gucci sunglasses (Benedict XVI).
If tabloid covers are any indication, one’s appearance is more important than jewelry, most people preferring to look like a supermodel than the Queen of England. Perhaps jewelry has been, by necessity, a substitute for cosmetic surgery, even a distraction. Is cosmetic surgery the 21st-century extension of jewelry? One of my patients called her cosmetic surgery her “everyday jewelry.” The late (and always witty) Joan Rivers justified the cost this way, “Better a new face coming out of an old car than an old face coming out of a new one.”
Having a facelift is really just an extension of one’s desire for self-improvement—to look one’s best. The psychological benefit can be profound. Fully 83% of our patients report an improvement in self-esteem afterward (Swanson E. Outcome analysis in 93 facial rejuvenation patients treated with a deep-plane face lift. Plast Reconstr Surg. 2011;127:823–834). Many of my patients are also losing weight, exercising, quitting smoking, eating better, having cosmetic dentistry, whitening their teeth, undergoing Lasik vision correction, and having their varicose veins injected.
The traditional view is that a facelift is not supposed to be undertaken in response to an external life event and there should be no expectation that a facelift will solve one’s problems. It may be more accurate to say that antiquated methods have simply not been up to the task.
In truth, many patients do experience a psychological improvement from cosmetic surgery (89% in our survey, referenced in the preceding paragraph). It is not unreasonable for them to think that surgery may have a positive effect on their quality of life. I’ve been told by many of my patients, including patients who are also psychologists, that a few hours of surgery were more helpful in boosting their self-esteem than hundreds of hours of psychotherapy.
Life events may well trigger a patient’s decision to have cosmetic surgery. The example I see regularly is the woman whose husband left her for a younger woman. That an aging appearance should be the basis for a marital breakup speaks to the power of physical appearance. A youthful appearance alone can trump all the advantages of staying together—shared life experiences, memories, and children. Plus the tremendous personal and financial upheaval that results from divorce. Obviously, there may be other considerations, but undeniably lost youth is a big one.
The good news is that expertly performed plastic surgery can help a woman “ramp up” her appearance, her self-esteem, and help her to make a new start. Nothing frivolous about it, cosmetic surgery can have huge practical implications for the direction her (or his) life takes.
The Workplace
I am struck by how many of my patients tell me that work pressures are part of their decision to have surgery. They say that while there is no official age policy where they work (not surprisingly), there is an unofficial one. If this were not the case, why is it that early retirement is offered and encouraged for employees over 55? A major telecommunications employer based in Kansas City settled a multimillion-dollar lawsuit brought by its older employees, including patients of mine, who were let go because of their age. Although both sexes are affected, the pressure can be greater for women.
Typically these patients are about 55 years old and feel they are on the cusp of being “over the hill.” They may very well lose their job to a younger employee. Often being older is not so much the problem as looking older. Although it is shameful to treat older, experienced employees this way, it is also a reality. Patients tell me there is no fighting it. Age discrimination is a sad commentary on our values, but a bias that is unlikely to change. My own mother told me that if she had not had a facelift at age 58 (yes, I did it), she would not have been able to stay on and eventually retire from full-time employment at a time of her own choosing, which was 67. Usually thought of as personal and discretionary, cosmetic surgery can sometimes have a very practical function—keeping people in their jobs.
How Young Will I Look After a Facelift?
Surgeons often claim that a facelift will take a certain number of years off your appearance. A number I often hear at meetings is 10 years. Similar claims may be found in advertisements for skin cosmetics and laser treatments. With no scientific basis, these estimates are purely wishful-thinking. Photographs invariably show best-case results, with lighting, makeup, jewelry, and facial expression (often all of the above) more favorable in the “after” picture. These photos may be taken shortly after surgery, when swelling is helping to smooth wrinkles. These considerations do not include “photoshopping,” a practice that has become easy and widespread (and not used on any photos on my website).
The problem in analysis of results after facial cosmetic surgery is the pervasive, but incorrect, assumption that any changes are subjective and impossible to evaluate scientifically. How is it possible to quantitate change in apparent age? How much younger can you expect to look after surgery? We have some answers (Swanson E. Objective assessment of change in apparent age after facial rejuvenation surgery. J Plast Reconstr Aesthet Surg. 2011;64:1124–1131).
Apparent Age Reduction (Years)
Our Survey Says (71 Patients)
In our original study, photographs of patients taken before surgery and at least 6 months after surgery, without makeup under identical photographic conditions, and with no ancillary procedures after their surgery, were shown to members of the public who attended a Women’s Exposition. The “age guessers” were asked to judge the age of the person in the photograph, not knowing anything about the individual. Two different books of photographs were used, each alternating “before” and “after” photographs so that the age guessers did not view both “before” and “after” photographs of the same patient.
This study showed that the average reduction in apparent age after a facelift alone was 4.6 years. Patients treated with blepharoplasties were compared with patients without blepharoplasties; doing eyelid surgery, on average, provided another 2 years of reduction in apparent age. The same was found to be true for forehead lifts. Laser resurfacing, on average, provided 2.5 years of apparent age reduction. An interesting finding was that smokers’ apparent age reduction averaged 8.1 years, significantly more than nonsmokers (5.6 years), perhaps because they looked older to start with.
There was no significant difference when patients were compared by gender, decade of life (40s, 50s, 60s, 70s+) or body mass index. None of the 71 patients was judged to look older. The maximum reduction in apparent age was 14 years. Twenty percent of patients appeared a decade or more younger according to the impartial age raters. This study was the first to evaluate change in apparent age after cosmetic surgery. It is the first solid evidence that cosmetic surgery is effective. It was presented at the 2011 meeting of the American Society for Aesthetic Plastic Surgery.
Remarkably, surveys completed by the patients themselves (not the age raters) showed that 97% thought they looked younger after surgery and the average subjective age reduction was 12 years (range, 0–27.5 years), double the objective findings by the age raters (Swanson E. Outcome analysis in 93 facial rejuvenation patients treated with a deep-plane face lift. Plast Reconstr Surg. 2011;127:823–834).
How Long Does a Facelift Last?
This is one of the most common questions asked by patients. Almost everything in life wears out—the car, the washing machine, other body parts —so they want to know when their facelift will finally wear out too. They would appreciate a definite answer. But the answer requires an understanding of what a facelift does (reduce apparent age) and what it does not do (stop the aging process). By lifting and restoring tone to the face, a facelift can reverse many of the effects of time and gravity. Our study found that combined facial rejuvenation reduced apparent age by an average of 6 years, so a 56-year-old now looks 50. In 10 years, she will appear to be 60 years old, not 66. The facelift “turns back the clock.”
The aging process continues, of course, but the benefit of a facelift does not wear off at some future time. Women and men will always look younger than they would have without the surgery—6 months after surgery or 10 years after surgery. The comparison is really between their future appearance and how they would have looked without the benefit of surgery. Looking at it this way, the benefits are lasting.
So, when might a patient expect to return to have another facelift? If she is unhappy with the way she looks now and can expect to have a similar appearance in 6 years, it makes sense that she might return at that time for another facelift. However, many factors (including the patient’s expectations) influence this decision, and in some areas, such as the neck, the result at 6 years may still be an improvement on their preoperative appearance (See B.W. and B.K. Patient Photographs).
Periodic maintenance procedures after surgery can reduce subsequent changes of aging. Patients may return every few years for a light laser resurfacing, fat injection, commercial fillers, and Botox. With such maintenance (and sun avoidance), patients may look better in 6 years than they did before surgery. Some of my patients in their 50s and 60s believe they look better than they did a decade ago, and some fifty-somethings (See B.W., age 52, in Patient Photographs) even say they never looked better.
Some surgical improvements may persist beyond a decade. Double chins are an example. Fat removed under the chin does not come back, although the skin gradually loosens. Patients treated simultaneously with a chin implant have a permanently enhanced profile. The results of eyelid surgery may well last beyond 10 years. It is important for the reader to maintain a healthy skepticism of surgeons’ claims, including mine. For this reason, long-term follow-up photographs are included in the Patient Photographs section.
Redoing a Facelift
Most of us know of people who have had not just one facelift, but two or three. The perception is that these people must be unbearably vain. But this may be unfair. These people do not return for more surgery because they like having surgery. Rather, they return for more because the benefits have been lost or were not very noticeable to start with. Their early facelifts may have been “skin-only” procedures. Many mini-lifts are of this type. Such skin-tightening procedures can produce a “drawn tight” or “windblown” look. There is some early benefit after a skin-only lift, but this is followed by skin sagging only a few years later. The skin is notorious for its ability to stretch. This was the impetus for the development of deep-plane techniques that pulled tight on the inelastic connective tissue layer below the skin.
In fact, I have redone many such facelifts (See L.B. in Patient Photographs), some as soon as 1½ years after the original surgery. Even on some of my own patients treated using the more-effective deep-plane lift, I have reoperated to treat persistent jowls.
Fortunately, a facelift can be redone. The original scars are included in the skin that is removed. It is often possible to improve the scars by reducing tension on the earlobe and tucking the scars in closer to the ear and hairline to make them less conspicuous. The surgery proceeds much as a primary facelift does and, perhaps surprisingly, does not pose much greater difficulty for the surgeon (unlike a redo rhinoplasty). Usually a smaller amount of excess skin is removed, sometimes just the scar. The emphasis is on the deep-plane lift, which may not have been done before or perhaps not as extensively.
Avoiding Skin Tension
When operating on the face, it is important to avoid tension on the skin because the skin stretches easily. Most people have no trouble understanding this concept, and the reason for using another tissue handle (the SMAS) for elevation. One can hardly expect the skin to hold on its own (the same is true in breast lift surgery). It stretched out before and can be expected to do so again.
Restoring Facial Volume With Simultaneous Fat Injection
We now recognize that replenishing lost facial volume, the “refill” (one of the 4 R’s of rejuvenation) is just as important as tissue repositioning—the “redrape” provided by a facelift. A facelift alone is purely a repositional procedure.
Before fat grafting became popular, many plastic surgeons tried to manipulate existing facial fat, meticulously transposing one cubic centimeter (cc) of fat from the orbit into the “tear trough” (the curved depression that runs from the inner corner of the eye down onto the cheek, just where a tear would travel). Other surgeons have tried to pull up on the egg yolk-sized buccal (cheek) fat pad, which contains a measly 4 ccs of fat (about a teaspoon), using “suspension sutures” that don’t work very well in the first place. This is a tiny volume and the fat is likely to be flattened by the suturing anyway. Not surprisingly, it is difficult to see any volume or contour differences when I view the results presented at meetings. If there is a difference, it may be due to postoperative swelling on an early postoperative photograph. Photographs of patients treated with these fat-transpositional and suspension procedures do not meet my personal minimum standard for effectiveness—I have to be able to tell the “after” photographs from the “before” photographs without labels. One well-known early proponent (Dr. William Little) has abandoned suspension sutures.
To provide youthful facial fullness, introduction of fat harvested from another area of the body (such as the abdomen) is the key. This is the only way to truly restore lost facial volume. Rather than repositioning a few grams of fat from one part of the face to another, borrowing from Peter to pay Paul, it is possible to introduce a much greater volume of new fat, in quantities of 10, 20, 30, or more ccs. Fat injection represents the biggest advance in my facial rejuvenation surgery in the last two decades.
Even counting on some resorption of injected fat, say 50%, there is still a net gain, which is better than the zero net gain of any transpositional technique. To determine changes in volume after fat injection at the time of facelift study, patients at our center were studied with MRIs before and at various times after surgery. This study demonstrated a significant and lasting improvement in cheek volume. Patients studied showed an increase in cheek thickness at 1 month, and no significant loss at subsequent times (Swanson E. Malar augmentation assessed by magnetic resonance imaging in patients after facelift and fat injection. Plast Reconstr Surg. 2011;127:2057–2065).
The successful integration of fat injection with facelifting is an important advance in facial rejuvenation. However, not all plastic surgeons have embraced it. The usual explanation is, “I find the results inconsistent.” The irony is that few plastic surgical procedures can be counted on to produce fully predictable results and fat injection of the cheeks does provide lasting and consistent improvement.
Part of the acceptance problem may be that fat injection is perceived by many plastic surgeons as a painstakingly slow and tedious procedure. A facelift is already a meticulous and time-consuming undertaking, and surgeons may be tired after spending several hours already in the operating room performing a facelift and blepharoplasties. Although fat injection was originally performed using tiny quantities injected in tiny syringes, this method adds to the time commitment. Fat may be injected in larger volumes under low pressure, using atraumatic technique, without a need for centrifugation (I use the LipiVage system) and using fewer passes to reduce tissue trauma and swelling. This method means that fat can be injected in 30 minutes or less, making the technique an ideal adjunct to facelift surgery. Fat injection gives immediate, pleasing results and, by bringing new tissue into the area, improves skin turgor (fullness) and introduces thousands of stem cells, which research suggests may be highly beneficial to the surrounding tissue.
Separating Fact From Fiction
Perhaps no other plastic surgical procedure carries as much mystique as the facelift. A facelift is popularly understood as a renovation. The word is used loosely, even to describe makeovers of inanimate structures—“shopping mall gets a facelift.” For patients, though, the word “facelift” may conjure an invasive procedure that may radically change one’s appearance and not always for the better (a favorite subject of the tabloids). The negative impact of the word “facelift” is reflected in the facial expressions and responses from many of my patients after I recommend it—“Do you really think I need a facelift, doctor?” Much of my time in consultations is spent dispelling common myths about facelifts. Patients ask me about alternative procedures they have seen advertised that promise the results of a facelift but without surgery. By promoting products that have questionable antiaging benefits, these advertisers take advantage of the public’s fear of surgery.
Alternatives to facelifts are frequently presented in the media. The interviewed doctor remarks, “My patients do not want radical surgery.” It may not be disclosed that the physician being interviewed is a non-surgeon, perhaps a dermatologist, who does not perform facelifts. It is no surprise that he or she does not recommend them. Few operators recommend procedures they don’t perform.
It is true that there are many celebrities who look altered or unnatural, and some have been outspoken about their negative plastic surgical experiences. But there are many more who have been very pleased with their results and could not imagine passing up surgical options to keep their appearance from deteriorating. Performed expertly, a facelift can have a profoundly positive effect, as evidenced by patients testimonials and survey responses (Swanson E. Outcome analysis in 93 facial rejuvenation patients treated with a deep-plane face lift. Plast Reconstr Surg. 2011;127:823–834).
Patients need to be reassured that they will not look different, drawn tight or artificial after a facelift. They need to know they won’t look like they just stepped out of a wind tunnel. If these apprehensions can be relieved, they may very well decide to go ahead with a facelift. In my experience, the only way to alleviate these concerns is by showing results, before and after photographs of other patients. Not just one or two, but dozens.
Minimally Invasive Surgery
There is simply no substitute for a facelift. There is no other procedure that can effectively and consistently tighten the loose skin of the neck, eliminate jowls, and elevate the cheeks. Such minimally invasive procedures as “string lifts,” “thread lifts,” or “feather lifts” turned out to have negligible benefits and high complication rates caused by the permanent barbed sutures. They came on to the scene with much fanfare and then quietly disappeared. Ultimately the marketplace does not tolerate failure.
Alternative Procedures
Patients may ask about alternative procedures such as a “laser facelift” that avoid or minimize the incisions that come with a facelift. Laser skin resurfacing is a wonderful tool for smoothing wrinkles, fading brown spots, and even providing some skin tightening because of its “shrink-wrap” effect on collagen. But it does not lift the facial tissues or eliminate jowls, and the laser is not sufficient on its own to tighten the loose skin of the neck. These problems are squarely in the domain of a facelift.
Some operators advertise procedures that supposedly can deliver the result of a facelift, without the surgery. It is important for patients to know exactly what to expect from each procedure so that they don’t have unrealistic expectations or disappointments. Radiofrequency is being promoted as a nonsurgical alternative, but the results are modest at best.
Mini-lift
A mini-lift sounds attractive to patients—perhaps just the right combination of at least some surgical results and a minimum of downtime and expense. It is not a new idea. The first facelifts, performed in the early 20th century, were mini-lifts. However, because this maneuver is often little more than a skin-only procedure, it is less effective and less durable than a deep-plane facelift and only marginally less expensive. It is a lesser procedure that produces lesser results. It misses out on the advantages of a deep plane lift in treating the cheeks, jowls, and neckline to achieve a harmonious result that truly rejuvenates.
Furthermore, the mini-lift scar still courses around the ear. The scar is not much shorter than a facelift scar. It makes sense that if you are going to have such a scar, it is best to make the most of it and maximize the trade-off between a scar (the cost) and rejuvenation (the benefit). An equivocal results is not worth the time and expense.
Midface Lift
Occasionally, patients inquire about a “midface lift.” This term refers to the elevation of the cheek (malar fat pad). Some pioneering surgeons attempted to elevate the cheek using the same lower lid skin incision used to perform a lower blepharoplasty. It seemed like a good idea to try to make maximum use of this eyelid incision. But this approach did not work well in practice and, to their credit, the authors quickly alerted other plastic surgeons of its shortcomings.
Short Scar Facelift
“Short scar” procedures have an obvious marketing appeal. After all, who doesn’t want less scarring? The short scar facelift reduces the length of the scar behind the ear and may suffice in younger patients. But Dr. Daniel Baker, the author of this technique, cautions that older patients with loose neck skin are not appropriate candidates. Limiting the scar behind the ear may compromise the degree of neck skin tightening that may be achieved. Also, the abbreviated postauricular scar may cause skin puckering behind the ear (“dog ear”), a visible stigma of surgery. Further, only the portion of the scar that is normally well-hidden behind the ear is shortened. The more conspicuous portion of the facelift scar, in front of the ear, remains the same. When combined with an extended temple incision, the scar cannot be considered short.
MACS Lift
The MACS lift (short for “Minimal Access Cranial Suspension” lift), popularized by two Belgian plastic surgeons, has been adopted by some surgeons in the U.S. Although the technique is labeled “minimal access,” the zigzag scar may be conspicuous in the temple, where it can be visible along the hairline. Recognizing its limitations in treatment of the neck, the authors added an incision behind the ear. The incision now resembles a typical facelift scar and cannot be considered minimal. The lift relies on large, permanent “purse string” sutures placed in the SMAS, which is not undermined or released, so that its movement is limited. The lift relies on the sutures alone, which tend to loosen in the tissues over time. A variation on the MACS lift is the QuickLift, which makes use of a similar suturing method.
Lengthy Temple Incisions Are Unnecessary
Ironically, the “short scar” and MACS lift include lengthy incisions in the temples, which is the portion of the facelift scar which may be abbreviated without compromising the result, and a conspicuous portion of the facelift scar. It makes more sense to shorten the scar in the temple, where it is obvious, than behind the ear where it is usually is well-concealed.
In fact, the incision I use is no longer than the short scar and (original) MACS lift incisions—it is just positioned differently—shorter in the temple and a little longer behind the ear. Patients need to be able to wear their hair up and back, exposing their ears, without worrying about scars.
The author prefers the incision indicated by the blue line. Any incision in the temple (which is used in most facelift dissections, including the short scar and MACS lift) is avoided so as to eliminate a potential scar. Almost all women (and men) can wear their hair short or up without worrying about a visible temple scar. Swelling in this area gradually resolves. The “short scar” incision (black line) starts in the temple and ends in the crease behind the ear. This scar is longer in front, where it is visible and shorter behind the ear, where it is inconspicuous. Patients with loose neck skin require a longer incision behind the ear, indicated by the blue line. Fortunately this portion of the scar is usually well-hidden within the hair.
Scar Satisfaction
Our survey showed that 98% of patients were satisfied with their facelift scars (Swanson E. Outcome analysis in 93 facial rejuvenation patients treated with a deep-plane facelift. Plast Reconstr Surg. 2011;127:823-834). This high degree of scar satisfaction is reassuring, and allows the surgeon to use the procedure to maximum effect without being preoccupied by concerns about scarring.
The scar is the “cost” of this procedure and needs to be good enough so as not to outweigh the benefit. It does not take much scar deformity to negate a modest benefit in rejuvenation. Ideally, there is a substantial reduction in apparent age without a conspicuous scar. Marginal rejuvenation in the presence of a conspicuous scar deformity is obviously a net negative.
Complete Facial Rejuvenation
The 4 R’s of Facial Rejuvenation
The 4 R’s of facial rejuvenation are:
- Redrape (facelift)
- Relax (Botox or endoscopic forehead lift)
- Resurface (laser skin resurfacing)
- Refill (fat injection)
Many aging women have both saggy skin and wrinkles. They can benefit from both a facelift and laser skin resurfacing, so it makes sense to combine these procedures. Men tend to be more concerned about saggy jowls and necklines than about wrinkles, but they often elect to have other procedures such as fat injection or a forehead lift.
Most patients over 45 elect to have combined procedures. Plastic surgical procedures may be likened to paints on an artist’s palette. The more we have to choose from, the more lush the result. With many paints on the palette, we can often achieve dramatic results, providing a congruous, top-to-bottom facial rejuvenation. Once patients elect to have laser skin resurfacing and a facelift (which largely determine the length of recovery), other techniques can be added on without extending the recovery time or discomfort level, such as fat injection, eyelid surgery, and a forehead lift. Advantages of a single operation include a single recovery time and a single period of time away from work. Another advantage of combined procedures is the price. Plastic surgeons typically discount the price of additional procedures when they are done simultaneously. Of course, some patients prefer to start with one procedure. They may be nervous and need to develop a trust level with their surgeon. Or they simply need to prioritize financially and some things will just have to wait.
Safety of Multiple Procedures
There is no “safe” number of procedures. Typically, a single procedure, such as a facelift, involves more incisions, time, and tissue trauma than all of the other facial procedures combined. Combining procedures optimizes the result. However, combined procedures are not for all surgeons and not for the novice. Before undertaking combined procedures, the surgeon must be an expert in each procedure done individually and must do them regularly. Efficiency is mandatory to avoid excessively long operations. In my practice, operating times rarely exceed 6 hours. Any advantage of combined procedures is lost if the recovery is especially difficult.