INTRODUCTION
In considering laser skin treatments, the layperson is confronted by marketing hyperbole that is part and parcel of the business of cosmetic surgery.
Not All Lasers Are Created Equal
Anyone considering laser resurfacing is well-served with a basic understanding of the different types of laser treatments available, their pros and cons, and alternative treatments. The cost of not having this knowledge is that you may end up having a treatment of questionable value in our “buyer beware” marketplace. This is particularly true of treatments that advertise minimal recovery and no downtime. A healthy skepticism is your best defense.
Ablative Lasers
The Ultrapulse laser was introduced to me in 1995 at a meeting in Marina Del Ray, California. Pioneering physicians, plastic surgeons, and dermatologists had started using lasers to “resurface” the skin. Although lasers had been used in medicine and surgery for a few decades, they were too powerful to use on surface wrinkles. The aptly named “Ultrapulse laser” was adapted so that it would fire very short bursts of energy, enough to vaporize the surface layers without harming the deeper skin cells. Although I had arrived at this meeting with a degree of skepticism, wondering if the use of lasers on wrinkles was a more for marketing than for getting results, the theory seemed reasonable and I looked forward to seeing how it would work in practice.
Shortly after treating my first patient, I realized that this treatment offered a safe, effective treatment for wrinkles and skin blemishes that could be done at the same time as other procedures such as eyelid surgery (blepharoplasty) and facelifts to produce overall facial rejuvenation. I started using it in my practice cautiously, doing a single “pass” or two with the laser, thinking that I could always do more and wishing to avoid any complications. In fact, this conservative approach turned out to be the correct one and remains unchanged in my practice today.
Result vs. Recovery Time
For patients contemplating laser resurfacing, the question becomes, What is more important, a more impressive result or a shorter recovery time? Local anesthesia or I.V. sedation? For many of my patients, who wish to do this once if possible and not return for a long time (“nothing personal, doc”), the result is their priority. A few days more recovery time is an acceptable trade.
Of course, this preference for results may be affected by the surgical orientation of my practice, compared with, for example, a dermatology office. I often perform surgical procedures simultaneously with laser resurfacing (fat injection, for example), and I am fortunate to have easy access to an on-site surgery center and anesthesia.
The Importance of Epidermal Treatment
The fully ablative laser treats the epidermal damage, which is a continuous problem, in a continuous fashion, while also producing skin tightening because of the thermal effect in the dermis below—two hits already. The advantage and disadvantage of the fractional laser is its noncontinuous ablation of the epidermis, which allows faster healing but compromises the epidermal result. As the fractional CO2 laser becomes more ablative, it approaches the effectiveness of its fully ablative predecessor, but there is less advantage in healing time. The comparison is no longer between a lunch-hour procedure and a week off work. The difference in recovery time is reduced to several days.
Laser recovery time becomes a moot point in patients who are having other procedures, such as a facelift, simultaneously. They won’t be looking presentable for at least a few weeks anyway. To obtain the best epidermal result and make the most of my patient’s precious recovery time, I prefer the ablative CO2 laser, but I typically make only one or two passes. I want my patient to recover quickly. I still want my cake and eat it too.
Making a Decision About Laser Treatments
Many patients are willing to accept a reasonable downtime provided they get results. This is particularly true for patients who are having other procedures such as blepharoplasties (eyelid rejuvenation) or facelifts, who have prepared to be off work for a couple of weeks anyway.
A litmus test for incorporation of a technique in my practice is that I have to be able to tell the “before” pictures from the “after” pictures. It is unrewarding for a physician to have a patient comment, “I don’t see a difference.” More important, it is unrewarding for the patient, who has gone to some trouble and expense. Unfortunately, there is a long list of treatments with results that are marginally effective. Less is less. Patients may grumble about the recovery phase, but it’s better to grumble about that than about no results. Ablative laser resurfacing works, and the benefits in terms of less wrinkling and age spots can last for years.
PATIENT PHOTOS
S.I., Age 43
Procedure: CO2 laser resurfacing, upper and lower transconjunctival blepharoplasties, excision of facial skin lesions, and endoscopic forehead lift.

Before, 6 months after
J.A., Age 44
Procedure: CO2 and erbium laser resurfacing, upper and lower blepharoplasties, fat injection (29 cc), and endoscopic forehead lift.
Before, 4½ months after
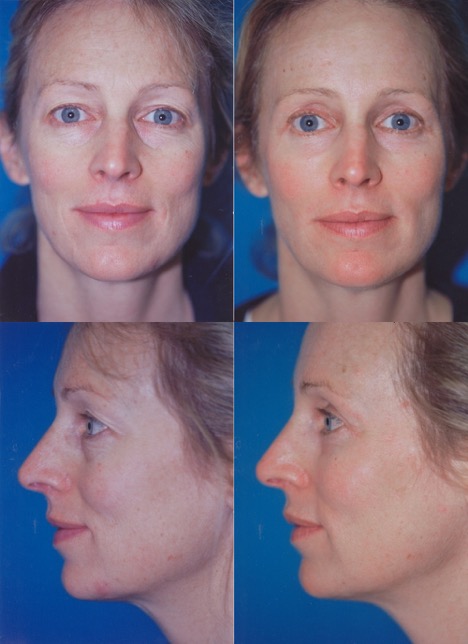
V.L., Age 45
Procedure: CO2 laser resurfacing and fat injection (46.5 cc).

Before, 3 months after
B.D., Age 82
Procedure: CO2 laser resurfacing, facelift, submental lipectomy, and biopsy of facial skin lesions.

Before, 2 months after
How It Is Done
Is Laser Skin Resurfacing “Surgery”?
Although there is no scalpel, laser resurfacing does break the surface of the skin. Any treatment that removes a superficial skin layer does count as “invasive.” Although there is marketing trend that emphasizes (translation: capitalizes on) the expression “noninvasive,” this term is often synonymous with “noneffective.”
Laser Skin Resurfacing and Anesthesia
Although I treat partial facial areas under local anesthetic alone, with the patient awake, my preference is to use a brief intravenous sedation. If the full face is to be treated, it is most comfortable for the patient to be asleep.
Laser Precautions
Laser precautions are taken. These include lubricated metal eye shields that provide complete eye protection.
How Long Does the Procedure Take?
The procedure does not take long, usually about 15 minutes. It is almost embarrassingly easy to do and to teach. The art of resurfacing is in knowing how many passes to use on the different areas of the face, which have varying skin thicknesses, and how to vary energy levels and passes with the laser in patients of different ages and complexions. This knowledge comes with experience. Inexperienced operators or those that do not have a medical background are at a disadvantage.
Advantages of Full Face Treatment
When physicians first performed laser treatments, we often did “spot treatments.” Today, it is much more common to treat all of the face. We can go deeper where necessary, usually around the mouth where there are deeper lines, and more superficially over less wrinkled areas such as the cheeks. The facial skin is evenly and uniformly treated. There is no need to apply makeup to blend in the red areas with the surrounding untreated skin until the redness fades. All of the skin has the same glow and all of the facial skin benefits, not just individual sections.
What To Expect After Surgery
The face is swollen and red. There is seeping from the skin because the skin has temporarily lost its barrier function. The fluid that oozes from the skin is yellowish and forms crusts. Washing regularly helps remove these crusts. However, it is unnecessary to completely remove the crusts. They come off when they are ready. Vaseline ointment is used to keep the skin from drying out. Usually the skin is healed and no longer oozing about 5 to 7 days after the laser treatment.
Once the skin is healed, patients can use sunblock and apply makeup to help hide the redness. You can tell the skin is healed when it is pink rather than red, is no longer “raw,” and is not oozing anymore. Also, once the skin is healed, patients can use a moisturizer and stop applying Vaseline. Petroleum jelly is a great skin lubricant, but it is messy, gets in the hair, and can clog skin pores, so you don’t want to continue it longer than necessary.
Some areas heal more quickly than others, depending on the depth of the laser treatment. Usually the lower eyelids, crow’s feet, and the skin around the mouth take a little longer to heal than the forehead and cheeks. For a few days, patients may apply Vaseline to these areas and a moisturizer to the healed areas.
Normal Findings After Laser Resurfacing
Side effects expected after treatment include:
Redness can take up to several months to resolve fully after CO2 laser resurfacing. Patients may appear to have a sunburn and then a healthy glow that can be toned down with makeup. Spot treatments leave circular red areas that are more noticeable because they border untreated skin, which is why I usually treat the whole face. Also, there is no reason to leave out areas of the face that can benefit. After all, there is no area of the face that is not exposed to photoaging from sun exposure.
Swelling: A small degree of swelling is not objectionable. Swelling helps smooth out lines and looks youthful. Photographs taken shortly after laser resurfacing can show results that are exaggerated by swelling. For this reason, it is helpful to look at photos several months after treatment, so that the temporary effects of swelling have resolved and the true benefit can be assessed.
Oozing of the facial skin is due to the temporary loss of the normal skin barrier function. The oozing stops when the skin is healed, usually by 1 week after surgery. Some areas take longer to heal than others, such as the orbital rims and around the mouth, where more passes may be used to treat deeper lines. Patients often report feeling much better when the skin is healed.
A burning sensation is caused by sensory nerve trauma which produces burning or stinging sensations. It is important to keep the skin from drying out. Hydrocortisone cream (1%), available over the counter, can also relieve itching or stinging. An oral antihistamine such as Benadryl is also helpful and can provide some needed sedation, particularly at night.
Complications
Complications are not considered normal but do happen. Patients need to be informed about possible complications so they are not surprised if they experience one (or more). They include:
Infection.
I favor the open (no dressing) technique for laser resurfacing because this allows the face to be washed frequently and reduces the likelihood of bacterial colonization, which could give rise to infection. Some patients do not cleanse adequately after laser resurfacing. They are tentative and worry that maybe they will scrub too hard and it can be painful during the first few days. Close follow-up is important to be sure that patients are cleaning properly. We typically see our patients in the office the day after laser resurfacing to make sure that they are cleansing the face properly. We often prescribe a short course of antibiotics and Valtrex to help prevent bacterial or viral infection. With regular facial cleansing, the likelihood of infection is very small. Infectious bacteria simply don’t have an opportunity to colonize the skin. The face has an excellent blood supply and resists infection unless colonization is allowed to develop. If an infection does occur, it will likely respond to frequent cleansing and antibiotics.
Hyperpigmentation.
Laser resurfacing can cause the pigment cells in the deep layer of the skin (melanocytes) to produce extra melanin which causes darkening of the skin. Hyperpigmentation is more common in patients with naturally darker skin types and is also much more likely to occur in the presence of ultraviolet light. Because the pigment cells are sensitized to UV light by laser resurfacing, it is very important to protect the skin from ultraviolet light after treatment. Sources of UV light include natural sun exposure and tanning beds. Our patients are regularly reminded after surgery to protect their skin and regard the sun as the enemy. For several months after laser resurfacing, and at all times when the skin is still red, patients must protect their skin from UV light. They need to regularly apply sunblock while outside and even in the car. A broad-rimmed hat and a large pair of sunglasses are especially helpful. I recommend at least 6 months of sun protection. Of course, it’s a good habit to get into anyway because UV protection reduces future photoaging.
If hyperpigmentation does occur, it is treatable. The most important treatment is avoiding the cause—ultraviolet exposure. A bleaching lotion (hydroquinone, 4%) may be prescribed to reduce the output of melanin by the pigment cells. But no amount of bleaching cream can overcome the effects of the sun if the skin is unprotected. The bleaching cream is applied in the evening to the darker areas, avoiding the lighter skin. The cream has a shelf life of about 2 months, so the prescription needs to be refilled if longer periods of treatment are needed. The importance of UV protection is one reason laser resurfacing is popular in the winter months, particularly for patients with darker skin types.
Milia
Milia (whiteheads) can develop after laser resurfacing. This may be related to the use of petroleum-based ointments such as Vaseline to lubricate the skin after laser resurfacing. The openings of the sweat glands can be blocked and protein-containing fluid (sebum) gets backed up in the glands. Once the skin is healed, this ointment may be discontinued and a moisturizer can be used instead, preferably one that is not too greasy. For patients prone to whiteheads, “noncomedogenic” moisturizers are best. Whiteheads may be disrupted by vigorous scrubbing. It is not unusual for me to pluck these whiteheads at the time of follow-up appointments during the few months after laser resurfacing.
Allergic or Contact Dermatitis
An advantage of Vaseline over other ointments is that it is free of additives that might cause an allergic skin reaction. Neosporin ointment, triple antibiotic ointments, other ointments that contain antibiotics, and home remedies can sometimes cause an allergic reaction, characterized by redness, itching, and delayed healing. If any of these problems occur, it is best to discontinue the offending topical preparation, use Vaseline instead, and take an oral antihistamine.
Hypopigmentation
Laser resurfacing can interfere with the function of the pigment cells in the deep layers of the skin, causing them to produce less melanin, leading to lightening of the skin. This lightening effect can be helpful for patients with brown spots or unwanted darkening of the skin, such as dark circles below the eyes. Hypopigmentation, however, can also be a problem, particularly along the jawline, where the demarcation between treated and untreated skin can be conspicuous. Hypopigmentation is more likely to occur using the CO2 laser because the heat energy penetrates the skin more deeply, to the level of the melanocytes. This problem is reduced by bordering the laser treatment at the level of the midcheek instead of the jawline, where the skin is a little thicker and not as prone to hypopigmentation. Patients sometimes wonder why the laser treatment fades out over the cheek and not at the jawline, and this is the reason.
Care After Surgery
Getting Back to Normal
• It is normal for the face to be red and swollen after surgery.
• Wash your face with mild soap and water, starting the morning after surgery.
• Use a soft cotton washcloth and don’t be afraid to rub on the areas treated with the laser. This helps take off the surface crust and prevent infection. Don’t worry if there is a little bleeding. Wash your face at least 3 times a day. Don’t be too tentative about washing.
• After washing, apply a thin layer of Vaseline to areas treated with the laser. The principles are easy: keep the skin clean, avoid infection, and avoid drying out the skin.
• You can tell when the skin is healed because there will be no more oozing and the skin will be pink. You can stop using the Vaseline and instead use a facial moisturizer at this point, usually 5 to 7 days after surgery. Typically the skin of the forehead and cheeks heals first, followed by the skin around the mouth and over the lower lids. Apply Vaseline to these areas and moisturizer to the cheeks and forehead. Sometimes, little whiteheads will form and these can be treated at the time of your office appointment.
• Avoid ultraviolet exposure after surgery. Regard the sun as your enemy at least until the pinkness has faded (and even afterward, to reduce the aging effects of UV light). The pigment cells are sensitized and will react to sunlight by creating more melanin pigment, causing unwanted hyperpigmentation. Wear a hat and sunglasses. Start using sunblock shortly after the skin has fully healed (usually within 7–10 days).
• If you feel a burning sensation, you can apply a cold washcloth.
• An oral antihistamine can be helpful to alleviate itchiness, such as Benadryl. But don’t take Benadryl at the same time as a prescription painkiller, because both products can cause sedation.
• Painful blisters are not normal and may indicate a herpes infection. Notify the doctor if this occurs.
FAQ’s
Q: How long have lasers been used?
A: Lasers are not new in medicine. They have been used for decades. In the 1990s, the carbon dioxide laser was modified to allow treatment of facial wrinkles, blemishes, and superficial acne scarring.
Q: How does it work?
A: The laser emits a very short (1/1000 of a second) burst of light energy that vaporizes the superficial skin layers, eliminating old sun-damaged skin cells. In response, new skin cells are created within the skin appendages (the sweat glands and hair follicles) that are located deeper in the skin. These new skin cells multiply and spread out over the surface, replacing old with new. New collagen is formed. The skin looks healthier under the microscope. The heat from the laser also makes collagen contract, tightening the skin.
Q: What areas can be treated with the laser?
A. Part or all of the face can be treated. The hands may be treated. The neck skin tends to be too thin and is not well-treated with laser resurfacing.
Q: Is it safe?
A: Because the burst of light is very short, there is minimal heat transmission from the surface to the lower layers of the skin. In fact, if you touch the treated area immediately after the laser treatment, it is not hot.
Q: Does skin color make a difference?
A: Yes, it does. Fair skin usually wrinkles more than darker skin. Fortunately, light skin responds well to laser resurfacing.
Q: Am I asleep for this?
A: Yes, in most cases, unless the treatment areas is small. A short IV sedation is ideal.
Q: What about other treatments such as chemical peels and dermabrasion?
A: Chemical peels use a chemical to cause a tissue injury to the skin rather than the physical vaporization produced by lasers. A chemical, often tricholoacetic acid (TCA) is painted on the skin. The chemical penetrates the skin. The body’s reparative process produces new collagen and skin cells, providing resurfacing. The problem is that it is difficult to know how deeply the chemical penetrates the skin. Not enough penetration and there is minimal benefit. Too much and complications develop. The laser is easier to control and more precise than chemical peels. It is the gold standard for resurfacing today. Studies comparing laser resurfacing with chemical peels typically favor laser treatment.
Dermabrasion causes a physical destruction of the top layers of the skin. A rotating wire brush is used on the end of a drill. It may be preferred by experienced plastic surgeons (and by that I mean older) to resurface the skin, although it is decidedly low tech. It is also messy, with blood splashing around in the operating room. In the age of lasers (and HIV), it seems primitive.
Q: What about “no downtime” lasers?
A: Nonablative lasers aim to stimulate collagen tightening without breaking the surface of the skin. However, the treatments are not as effective and usually have to be done in a series of visits. Patients are not typically enthusiastic about the results and may wonder whether the price was worth it.
Q: What about Thermage?
A: This treatment (Thermacool TC System, by Thermage, Inc., Hayward, Ca.) uses radio waves to try to stimulate collagen contraction in the deep layers of the skin. A cooling unit is used to avoid burning the top skin layers. The concept is intriguing. However, the treatments can be painful and results are minimal at best. There have been troubling reports of facial contour depressions from fat atrophy. Plastic surgeons’ experiences have not been positive and the technique has fallen into disfavor. This is a treatment that looks better on the drawing board than it does in practice.
Q: What about Fraxel?
A: The original Fraxel laser used a wavelength that did not cause much heating of the tissue surrounding the small laser holes, so there was not enough skin tightening.
Q: Does laser resurfacing help the neck?
A: The skin of the neck is different from the face. It is thinner and looser. Laser resurfacing must be done very cautiously, if at all. Usually the neck benefits most from a facelift. Any tightening from the laser treatment does not compare to what can be accomplished with a facelift. Laser resurfacing may be used occasionally to help smooth horizontal creases.
Q: Will I have a dressing on my face?
A: No. The open technique is preferred. This allows the patient to keep the skin clean and reduces the likelihood of bacterial buildup.
Q: Is laser treatment effective for acne scars?
A: Unfortunately, no treatment is very effective for acne scars. However, there may be some limited improvement. I tell my patients they need to be satisfied with a modest improvement, perhaps 25%. Simultaneous fat injection can help.